

Life is change
How it differs from the rocks.
I’ve seen their ways too often for my liking;
New worlds to gain.
My life is to survive
And be alive
For you.
You are the crown of creation
And you’ve got no place to go.
— Jefferson Airplane, 1970.
This week a young friend wrote to ask what’s the big deal about the virus. “More people die of other things,” she said. Gosh, I thought, maybe I should stop the presses on my latest book, Plagued, due out in October. After all, this pandemic is no big deal.
In the Maya Mountain foothills in early March, closing out a Belizean permaculture course and having meetings of experts about our plans for a Cool Lab microenterprise hub, I stayed up nights scouring the internet for then available science on the novel coronavirus. Based on that research, I put on mask and gloves, observed personal distancing while traveling, and quarantined myself for two weeks when I reached this island in Mexico, where I have been weathering the pandemic these past 20 weeks. I completed the Dark Side of the Ocean galley proofs and began work on a new book, specifically addressing what I was then learning — how best to have a decent life during a pandemic.
My research on Plagued gave me both a deeper understanding of this particular coronavirus and also better insight into the strange nature of the global response to it. In this multi-part essay, I will try to dissect some of those discoveries.
So how deadly is SARS-CoV-2? We still don’t know, but the more we are learning, the deadlier it appears. It is never a good idea to anthropomorphize a non-living snippet of nucleotides in a spiky protein shell, with no ability to eat, breathe, grow on its own, or make choices, but come on, this little guy really lends itself to the embodiment of some kind of malevolent monster.
Let’s review some of the new findings. We’ve known since January that the SARS-CoV-2 virus that causes Covid-19 disease is transmitted by tiny liquid droplets containing virus particles — a protein capsid enclosing a virion of serpentine, single-stranded RNA. These droplets, which may contain thousands of such virus particles, typically derive from the exhalations of infected people, but they might also come from toilet flushes, sweat, tears, blood, or any bodily excretions that can be aerosolized.
The finer the droplets, the longer they can linger in the air, and enclosed spaces like restaurants, public toilets, and elevators quickly become kill zones. Fomites, the droplets that land on surfaces, can also be picked up and ingested or absorbed, so it is good preventive practice to wash hands, launder masks, disinfect tables, chairs, phones and handles, and leave a UV-C light on when you are out (exposure to 250–270 nm UV-C light kills CoV-2 but also destroys endogenous microbial flora and can cause skin cancer).
Studies are showing now CoV can spread from people to animals and from dogs and cats (particularly cats) to other animals and potentially back to people. It does not (yet) infect farm animals including pigs, chickens, ducks, horses, sheep, and cattle. For dogs and cats, the primary symptoms are gastrointestinal rather than respiratory. The American Veterinary Medical Association and the CDC recommend that sick pets should be kept in quarantine, just as you would with people. If you are sick with Covid, or your pet is, avoid petting, snuggling, being kissed or licked, and sharing food. If you must come in contact with a sick pet, mask and wash your hands. They will likely recover, but in the meantime, they could be superspreaders (although no pet-to-human transmission has yet been confirmed). They should leave the home only on a leash or in a carrier.
Salunke, et al. The SARS-CoV-2 Virion and its Proteins

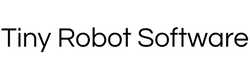
CoV-2 droplets infect by being inhaled or swallowed, where they attach to the linings of the respiratory system or the gastrointestinal (GI) tract, and following along those routes, the virus attaches itself to healthy cells (its spiky protrusions act like a key to unlock ACE2 receptors), cracks the cell nucleus, and rapidly reproduces itself by inserting its RNA virion into the cell’s DNA code. As cells die, they clog the lungs and other organs with necrotic tissue and fluids, leading, in the lungs, to Sudden Acute Respiratory Syndrome (SARS), as evidenced by low blood oxygen levels, difficulty breathing, and pneumonia-like cough, chest pain, and fever.
Induced inability to breathe is what makes waterboarding such an ineffective and sadistic torture. People will say or do anything to get it to stop. CoV-2 is a virus that has learned to waterboard.
By April, doctors around the world well understood that Covid was not just a lung disease. Many of the infected had lost their senses of taste and smell; in others, toes or fingers darkened as if bruised; hearts swelled; blood clotted; immune systems attacked organs they were meant to be saving. But because lessons were learned too late, doctors had been killing some of the patients they were trying to save. The virus employed some treatments used against it to strengthen its attack, like aikido. Intubate and turn up the airflow and viroids went deeper into the lungs. Flush fluids from the body in order to prevent lungs from filling and the virus crashes the kidneys.
The only surprise was that we were surprised. I write much of that off to Sinophobia, something both US political parties are comfortable superspreading. Nobody wanted to listen to Chinese doctors on the front line and many excellent early research findings were completely ignored until they had been replicated in the West months later: nasal swabs; putting patients on their bellies; administering remdesivir and anticoagulants; shutting down whole cities; mandatory masking.
Initially, WHO, CDC, and others said not to wear masks. The WHO made two mistakes. First, they didn’t realize scaling: if the probability of infection is p, if both people wear masks it becomes p squared. For example, if p=0.50, both people wearing a mask would lower p to 0.25. Second mistake: if I reduce the viral load by half, I don’t decrease probability of infection by half — I may decrease it by 99%. That’s because the probability of infection is nonlinear — it’s an S-curve. In addition, they lied because they were worried about a mask shortage.
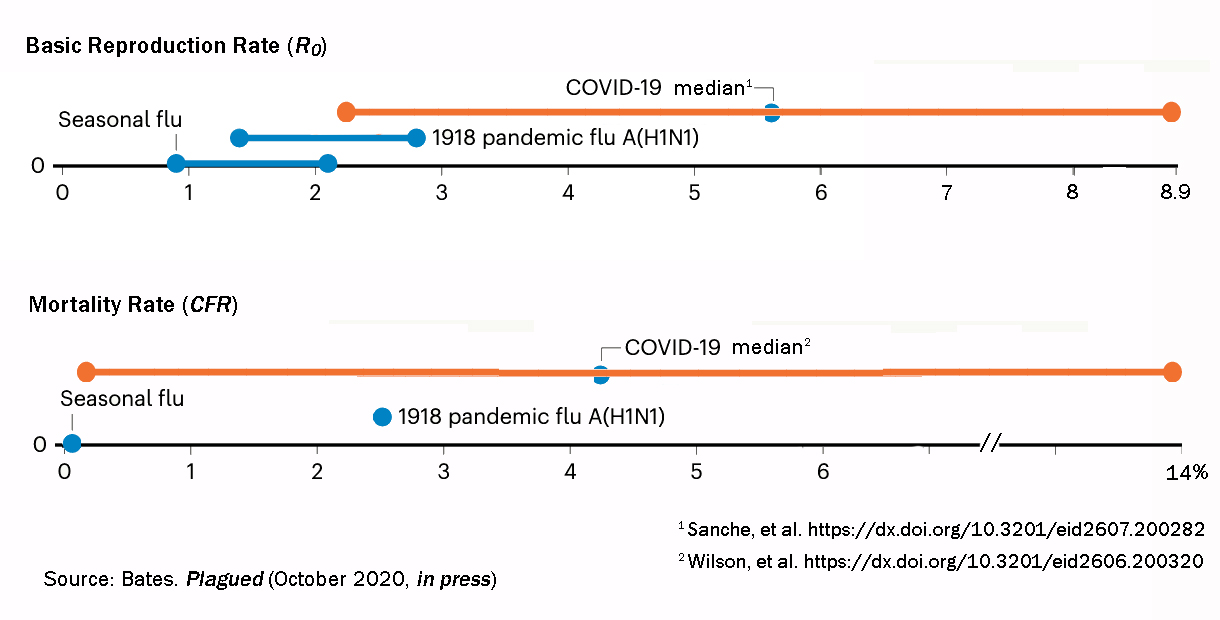
Mortality rates from the first quarter of 2020 left epidemiologists scratching their heads about how deadly CoV-2 is. The Case Fatality Rate was nearly 14 percent in Italy, but only 0.5 percent in Iceland. Germany and Spain were 4.5 percent, and South Korea half that. The United States mortality rate is currently 6 percent, but because testing is so poor, it could be lower. Or, because hospitalization requires insurance, which is tied to employment, it could be higher. The global average now is 6.8 percent, with a median of 4.2.

Lethality depends on a whole host of factors that vary from country to country, city to city, and person to person. We can see by comparing total deaths in a given city over the past several years that the first half of 2020 made a sharp mortality-by-all-causes spike, geographically mirroring local outbreaks. Total anomalous deaths are well above confirmed Covid deaths, leading to a suspicion that most Covid deaths go unreported. Extrapolating from those numbers, 150,000 deaths in the US could actually be 1.5 to 3 million. Epidemiologists have predicted one million US Covid deaths eventually. One million could have been surpassed last month.
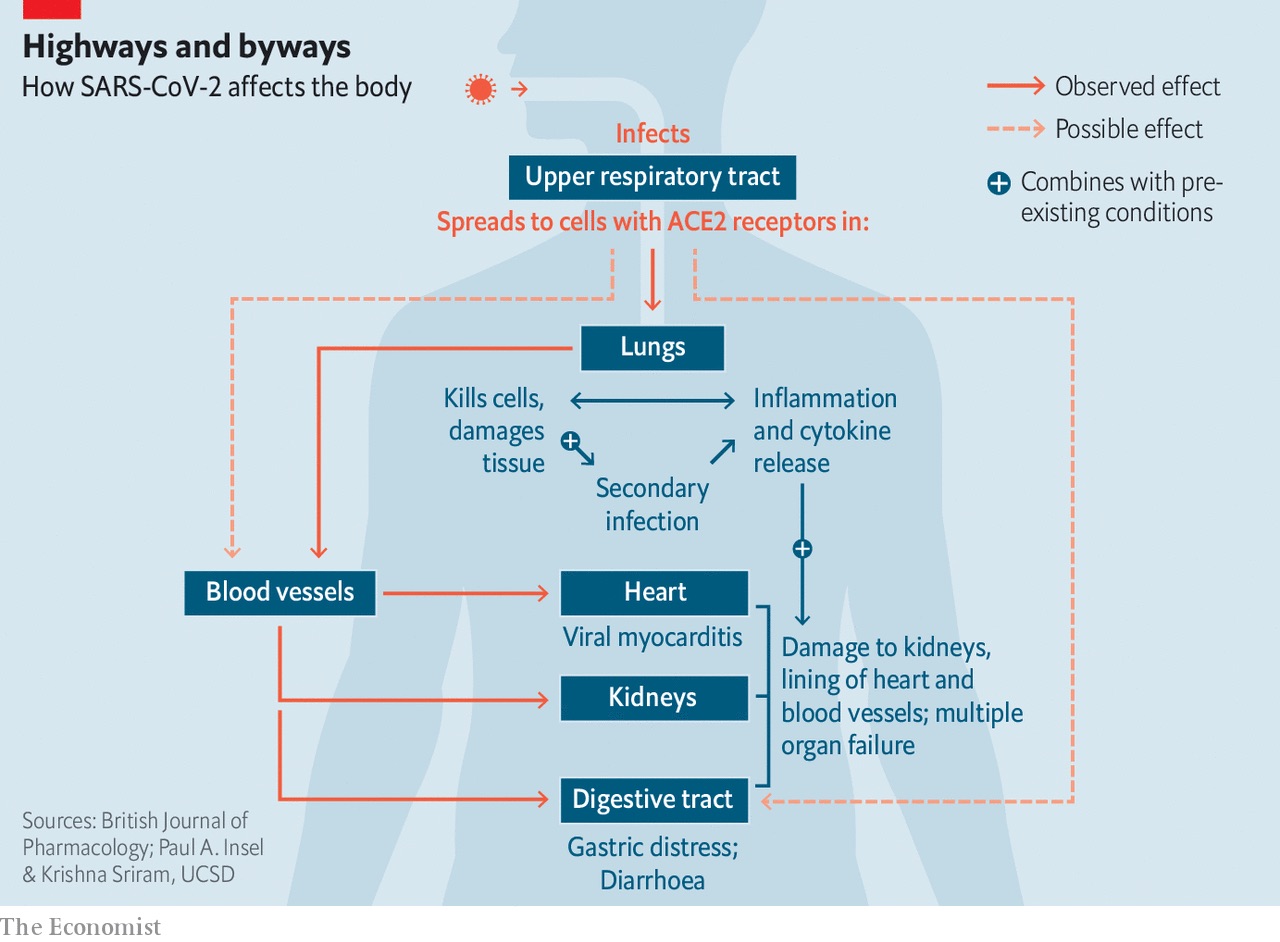
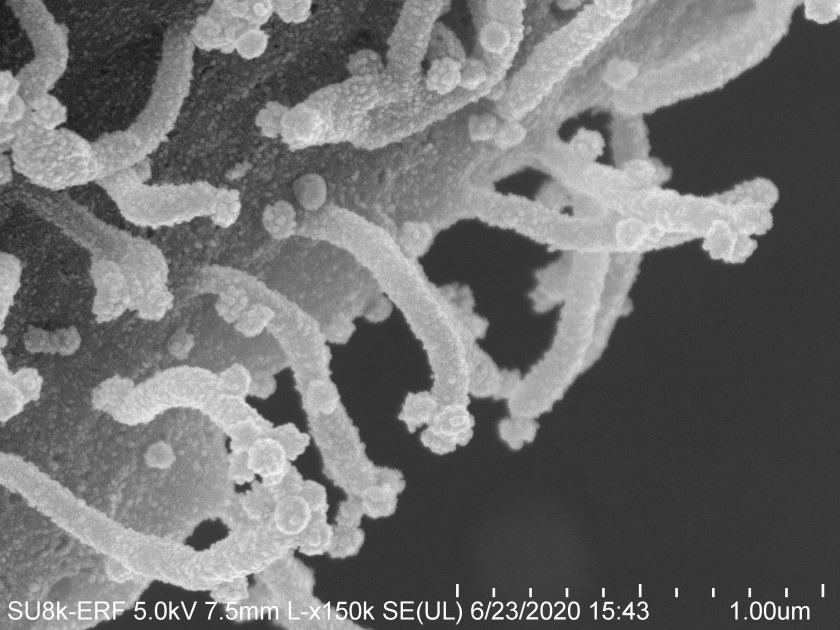
In January, Chinese scientists mapped Covid’s attack route into vascular endothelial cells through the Angiotensin-Converting Enzyme #2. ACE2 is found as a coating on cells in the upper respiratory tract and lungs, as well as on the heart, kidneys, and intestines. When a CoV-2 virus particle hacks a cell’s genome, it instructs the host to sprout sticky filopedia that extend out into the bloodstream like flypaper, glomming more virus particles passing by in the blood. CoV-2 devastates its target by concentrating firepower.
Filopedia microscopy by Dr. Elizabeth Fischer of NIAID/NIH
We know that ACE2 receptors are also in cells of kidneys, pancreas, gallbladder, intestines, testes, and in the nose’s olfactory cells. While Covid patients were 2.6 times more likely to have fever or chills, 2.2 times more likely to have trouble breathing or be coughing, and twice as likely to have muscle aches, they are 27 times more likely to have lost their sense of smell. That’s all about ACE2 receptors.
 The diarrhea, nausea, and abdominal pain that about one-third of Covid-19 patients experience is a viral attack on cells of the lower GI tract. Last month, scientists studying 1,000 Covid-19 patients at a New York City hospital reported that 78% of those in intensive care developed acute kidney injury. A quarter of covid-19 patients in British ICUs had kidney problems severe enough to require dialysis.
The diarrhea, nausea, and abdominal pain that about one-third of Covid-19 patients experience is a viral attack on cells of the lower GI tract. Last month, scientists studying 1,000 Covid-19 patients at a New York City hospital reported that 78% of those in intensive care developed acute kidney injury. A quarter of covid-19 patients in British ICUs had kidney problems severe enough to require dialysis.
We now see the virus attacks platelet-producing cells, called megakaryocytes, in the lungs. This can cause extensive clotting in the veins and other small blood vessels of patients’ hearts, kidneys, liver, and lungs. Black and brown skin as a higher co-morbidity indicator may not be entirely a function of social injustice. Inherited red blood cell irregularities such as sickle-cell anemia can be exploited by Covid to starve the blood of oxygen.
Seven to 31% of patients with severe Covid have a high incidence of cardiac arrest and arrhythmia. In part that is due to the extreme inflammatory response, but in part it is because ACE2 receptors line the inside walls of capillaries, which CoV-2 can clot, causing blue extremities, too little blood flow to the gut, and cardiac arrest.
With the number of Covid patients closing in on 20 million, epidemiologists hope the virus has no more surprises in store. But they’re not counting on it.
Cytokine Storms
The Spanish Flu of 1918 killed young healthy people more than children or the elderly because it caused an overreaction of the immune system to the infection. As the body’s own killer cells attacked healthy cells the condition quickly became fatal. Same with HIV/AIDS. Same with Covid.
George Freeth from Wikicommons and Lynn Shelton by Stuart Isett NY Times
 My friend and mentor the “lunatic farmer” Joel Salatin spouted on his blog for months that Covid could be beat just by building a good immune system through a nutrient-dense diet and regular exercise. Others have said the same, but they are wrong. I recall the death of Irish Hawaiian George Freeth who introduced surfing and lifeguarding to California 100 years ago. It is difficult to think of a healthier human specimen, and yet he was felled at age 35 by a cytokine storm from the Spanish flu. I can’t help but wonder whether Marc Maron’s romantic partner, filmmaker Lynn Shelton, who died suddenly at age 54 in May of “acute leukemia” was in fact the victim of a Covid cytokine storm — a white blood cell tsunami — and how many like her are similarly misdiagnosed.
My friend and mentor the “lunatic farmer” Joel Salatin spouted on his blog for months that Covid could be beat just by building a good immune system through a nutrient-dense diet and regular exercise. Others have said the same, but they are wrong. I recall the death of Irish Hawaiian George Freeth who introduced surfing and lifeguarding to California 100 years ago. It is difficult to think of a healthier human specimen, and yet he was felled at age 35 by a cytokine storm from the Spanish flu. I can’t help but wonder whether Marc Maron’s romantic partner, filmmaker Lynn Shelton, who died suddenly at age 54 in May of “acute leukemia” was in fact the victim of a Covid cytokine storm — a white blood cell tsunami — and how many like her are similarly misdiagnosed.
When infections occur, they activate two parts of the body’s immune response — “call to arms” genes and “call for reinforcement” genes. The first group produces interferons that act like mountaintop signal fires. They cue neighboring cells to activate defenses. These neighbor cells buy time for the second group of genes to produce proteins called chemokines that emit a biochemical “help!” alarm. When distant antibody-making B cells and virus-killing T cells — the immune system’s hunter/killers, the cytokines — sense that alarm, they race to the site and start shooting down viruses like a video game of space invaders.
But here is where Covid gets scary. Children might want to leave the room now. SARS-CoV-2 blocks the neighborhood watchtower gene while at the same time overstimulating the call for reinforcements. Once it hacks the genome of its first cell, it makes a protein that blocks that cell from warning its neighbors. It fells the watchtower. There are no limits to replication for at least the first few days. When cytokines do arrive, they come in such panic numbers that they produce a storm of inflammation at the infection site. That induces a runaway cell destruction that kills the patient.
New Normals
Writing for the online journal MedPage on July 27, Dr. Fred Pelzman, a recovering Covid patient himself, said:
Many patients who suffered severe pneumonia are still in the recovery phase, with prolonged fatigue and ongoing dyspnea. They tell us they are still “not themselves,” and have a sense of constriction and pulling to their breath. More than likely, as symptoms persist, we will start to evaluate these patients further, with repeat chest imaging and pulmonary function tests.
We may as yet discover what kind of lung disease this is, this residual damage, and whether it responds to medications for asthma or COPD or maybe something else. Or maybe just gradually resolves. Or maybe leaves some people with chronic damage and deficits.
I’ve seen a few patients who have residual loss of their sense of taste or smell. For me, while for a few weeks there I could barely smell or taste anything, now 4 months out I’ve noticed that some of my favorite foods just don’t taste the same, that many foods have lost the depth of flavor I’m used to tasting, and that certain smells, from my aftershave to my morning cup of coffee, are even bordering on the newly unpleasant.
I’ve had patients tell me their OCD has ratcheted up, their anxiety medicines are not working, they find themselves crying all the time without any other symptoms of depression. One patient told me that she’d noticed that she could no longer do math in her head. Something as simple as calculating the tip at a restaurant, which used to be incredibly easy for her, now was something she had to slowly and methodically work out.
Another interesting type of clinical presentation that I and a few colleagues have seen, although we’re not sure if this is a definitive syndrome or not, has been patients, several months out from recovery from their Covid-19, calling up with a panic that they now feel the exact same symptoms they had when they became sick initially. We’ve seen a few patients who’ve had the exact same clinical presentation as before, feeling feverish, diffuse body aches, cough, even a few patients who feel they’ve noticed a change in their sense of taste or smell.
As we evaluated them, we feared that we were seeing that thing we all dread so much, the definitive evidence that patients can get this disease twice. Luckily, all of the repeat swabs on these few cases we’ve seen have come back negative, and interestingly, once the swab results came back, the symptoms rapidly abated in most of these patients. Is this some form of post-traumatic stress response, or some underlying residual inflammatory process that may get reawakened, or reactivated as antibody levels drop off?
Virologists cannot yet say that CoV-2 antigen immunity, once established, persists, which is to say we don’t yet know if you can get Covid a second time, or a third; whether it is worse the next time; whether blood-derived vaccines would work in that case; or therefore, whether there is even the possibility of “herd immunity” or vaccination.
A survey of the Spanish population published July 6 in The Lancet found that 95% were seronegative to SARS-CoV-2 infection (had no antibodies), even in hotspot areas, despite many of the same individuals having tested positive before. It found that 14% of persons who had previously developed antibodies no longer had them a month later. Ian Jones, a professor of virology at the University of Reading, said, “Anyone who tests positive by antibody test should not assume they are protected. They may be, but it is not clear.”
“But these concerns are confused and mistaken,” protested Yale immunologists Akiko Iwasaki and Ruslan Medzhitov in a July 31 New York Times Opinion, “… finding that naturally occurring antibodies in some Covid-19 patients are fading doesn’t actually mean very much for the likely efficacy of vaccines under development.”
That antibodies decrease once an infection recedes isn’t a sign that they are failing: It’s a normal step in the usual course of an immune response. Nor does a waning antibody count mean waning immunity: The memory B cells that first produced those antibodies are still around, and standing ready to churn out new batches of antibodies on demand.
Since no-one, not even the Chinese, can answer the basic question of immunity persistence yet, the only thing that can be said for sure is that Covid will be around for a while. This is not a second wave. It is not even the second inning of the first wave. This will not be going away by September. It will not likely be gone by the September after that. Covid could be something more like the Black Plague that showed up in 1346 and ended in 1353 after killing 30% to 60% of Europe’s population of the time. Or maybe it will be like the San Francisco plague of 1900–1904, which was followed by an aftershock in 1907–1908. Worst case: it is with us for the rest of the century, as Bubonic Plague was for the Ottoman Empire for the whole of the 18th Century.
If outliers like the USA, Russia, and Brazil were to follow the advice of other nations and take common-sense public health measures, even they could have Covid under control enough to resume much of the old normal in 6 to 8 weeks, according to epidemiologist Larry Brilliant.
That’s a moot point, though, because the United States will not begin behaving rationally any time soon. Next week we’ll look more at the implications.
This is the first of multiple parts.
Help me get my blog posted every week. All Patreon donations and Blogger subscriptions are needed and welcomed. You are how we make this happen. Your contributions are being made to Global Village Institute, a tax-deductible 501(c)(3) charity. PowerUp! donors on Patreon get an autographed book off each first press run. My winter book, Dark Side of the Ocean, is shipping out now. My next book, Plagued, should be out in a few months. Please help if you can.